Pandemic Progress Report: California & Australia, August 4

Pandemic Progress Report: Australia and Sacramento California, August 4
The SARS-CoV-2 pandemic is global, but it’s also intensely local. Every country, state, county, and community has its own history and trajectory. While the US has suffered in some ways from a lack of national leadership on the pandemic, in other ways the decentralization of decision-making has been a good thing as it accommodates different local conditions, and allows experimentation. So where are we today? Let’s look at my hometown of Sacramento, in California’s Central Valley, and also talk about what’s happening Down Under.
How many?
Since early June, community transmission of the coronavirus in Sacramento County has been on the rise. Trends for the most important metric–hospitalizations–have been steadily upward, until now.
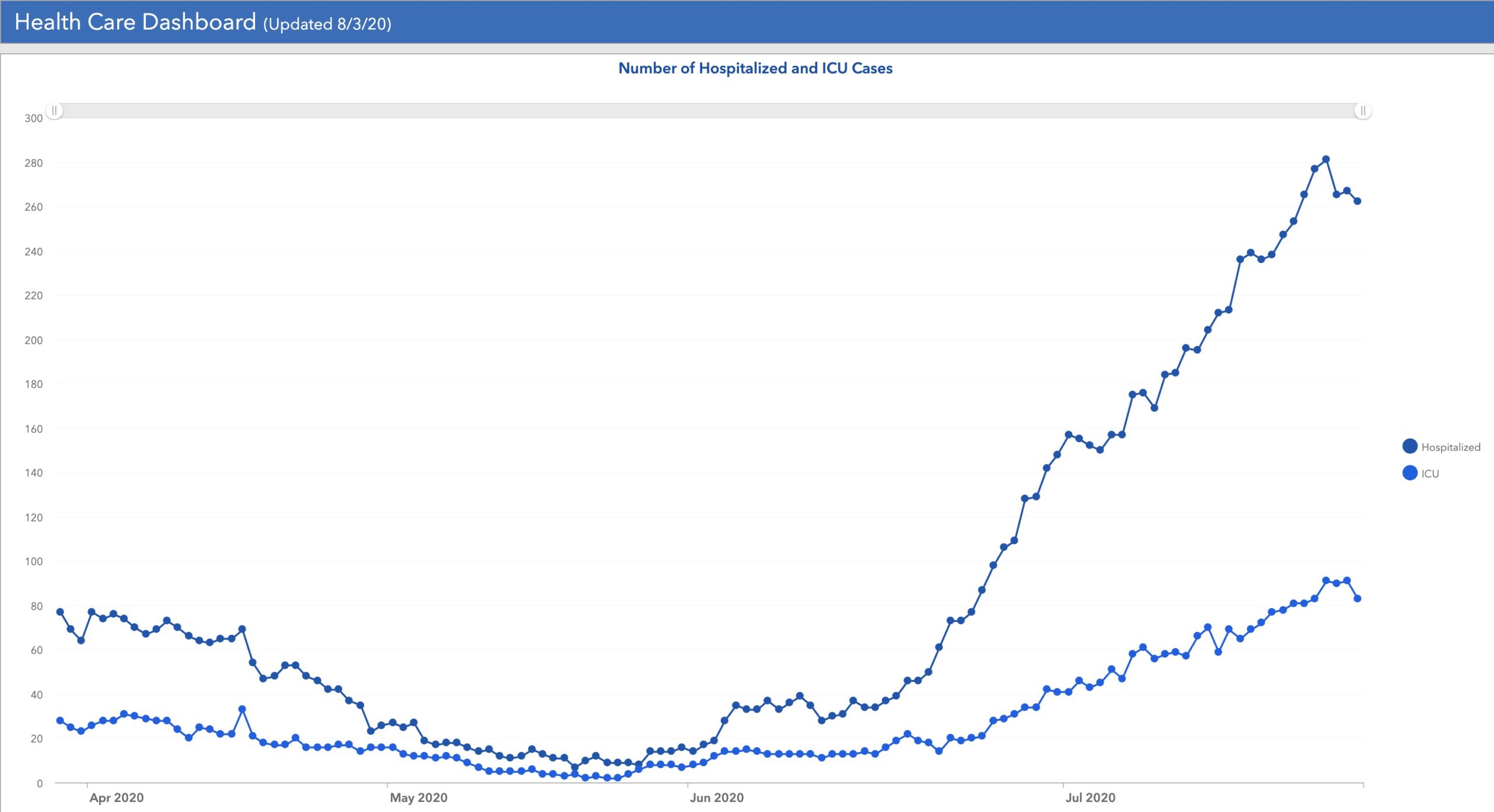
So far, Sacramento County hospitals have stayed within capacity for COVID-19 patients, although there have been impacts. I have heard about the infection finally getting to our Sacramento health care workers in more than sporadic numbers, and about hospital departments having to stop providing some services not to free up capacity (as was the case in April) but because of infections among the staff. Not all Central Valley hospitals have been so lucky. For example in nearby Lodi, CA, a hospital has had to summon military medical specialists from the Air Force to help staff their overwhelmed COVID ICU (source).
If that upward slope to the curve of COVID hospitalizations continues, we would be in trouble. However, we may have turned a corner. The downward blip of the past few days fits with the lag between case diagnosis and hospitalization. After peaking at troubling levels in early-mid July, new cases in Sacramento County have declined recently.
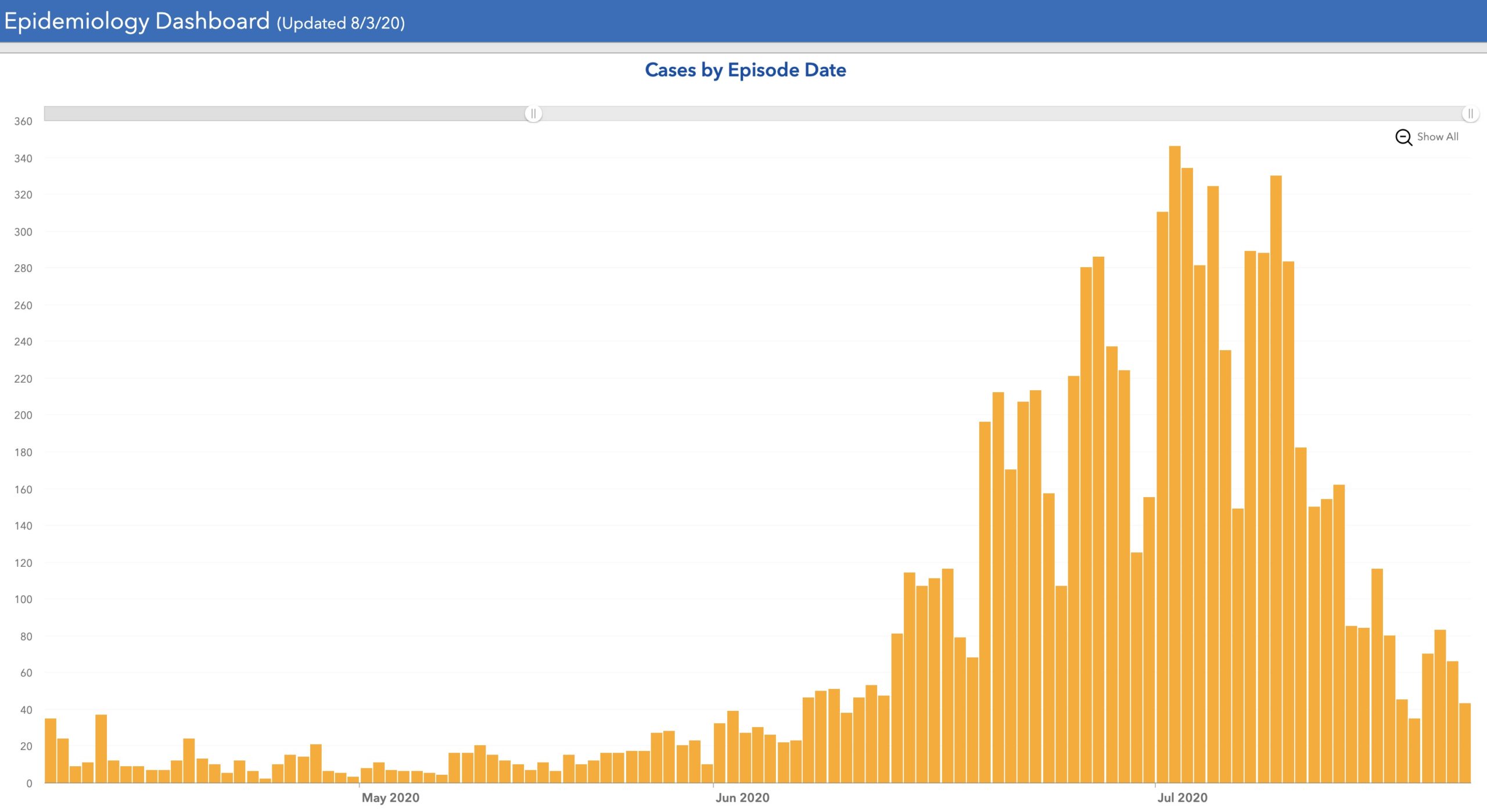
Sacramento County data source
Why the decline? First let me talk about another place with the opposite experience.
In a pandemic, all gains–and losses–are reversible
SARS-CoV-2 will probably be with us forever. The relationship between it and us will change as exposure or vaccination raises our collective immunity against the virus, but I expect this coronavirus to become a permanent fixture in our health, like seasonal influenza. In the short term, this means that countries or communities that get their infections down to a trickle are in a good but unstable situation. As long as the virus exists and people are susceptible to infection, the virus can come back from defeat. This is happening right now in a few places. Months ago, Australia and New Zealand crushed the curve. Using a severe nationwide lockdown (“even takeaway food and visits to intimate partners were off-limits”), New Zealand, a small, disciplined island nation entirely eliminated community transmission of the virus. At this time, “all restrictions have lifted on everyday life.”
Yes, you read that correctly. In New Zealand everything is back to normal. No masks, no social distancing, and all the schools and weddings you want.
But, “the country’s virus-free status is entirely reliant on strict border controls for returning travellers.” If mistakes are made, the island nation could backslide. That’s part of what has happened next door. Australia’s lockdown was milder but they also had great success in stopping community transmission. But the virus was never eliminated. All it needed was opportunity.
As Australians relaxed, infections came back. Now Melbourne, Australia’s second city (which, by the way, has a population comparable to the entire country of New Zealand), is reimposing “Stage 4” restrictions for six weeks. These restrictions mean “You are only allowed to leave your house for four reasons: shopping for food and essential items, care and caregiving, daily exercise and work” and “there is now a curfew on Melbourne residents between 8pm and 5am.” Furthermore, “Shopping for food and necessary supplies must be within 5km distance from your home, except if the nearest supermarket is further than 5km. Only one person per household can leave to go shopping per day. Exercise must take place within 5km of home, and must be in metropolitan Melbourne. Exercise is limited to one hour, once per day.”
So much for the proposed Australia-New Zealand joint travel bubble.
What happened to Melbourne?
For a more thorough analysis, read this. I have a personal theory that official, detailed government policies about what people can and cannot do have less impact than you would think. What really matters is the millions of individual choices people make. If I had a potential exposure will I voluntarily isolate for a while? Will I let my teenager hang out with friends in front of the TV, or force them outside? Am I going to wear a mask if it’s only for a few minutes? Each choice is small but their sum is large. In this light, the value of government-imposed restrictions is to set the tone and create a sense of urgency. My opinion is that Sweden is holding case numbers low because the collective actions of her citizens are greater than the official rules. Apparently in Melbourne, the collective actions of the citizens were less than the rules. A telling anecdote from the NYT article: “A door-knocking campaign to check in on 3,000 people who had Covid-19 found that 800 of them were not at home.” About a quarter of people who knew they were infected with the virus could not be bothered to stay in their homes! No wonder cases got out of control. Will people like this observe the new restrictions?
Which brings me back home to Sacramento. Infections have declined significantly since California Governor Newsom reimposed some restrictions on July 17th. Maybe banning indoor haircuts and dining helped a lot. Or maybe the restrictions–especially the ban on schools reopening until counties get off the state’s watchlist–got people’s attention again. Our individual behavioral choices matter. If we freely try to do our part to minimize spread of the virus, then our governments will have less need to impose mandatory restrictions.
Sustainability
Little New Zealand has won the pandemic so far. Good for them. Their initially extreme response succeeded, and they are in a sustainable situation. But complete elimination of local transmission was never a viable option for a country as large and open as the US. Our goal was and is to flatten the curve: to keep community transmission (the number of new cases) low enough to protect our hospitals, and allow for contact tracing. How strict do the rules have to be to achieve this? Depends on the willingness of the public to do their private best. Today in Sacramento I am hopeful that we’re headed in the right direction. Is the situation sustainable? Not until schools reopen for in-person instruction. Fingers crossed that will be achievable within a month.
The measures being enacted in Melbourne are unsustainable by any standard. Whether the Australians will tolerate the enforcement of the new lockdown for the expected six weeks remains to be seen. I know it would not fly in most parts of the US at this point. Australia is trying to beat back the virus to the low level they previously enjoyed. The US is apparently willing to accept much higher rates of transmission. What does this mean for the medium term (3-6 months)? I’ll be writing about herd immunity soon.
———————————————–
Other Data of Interest
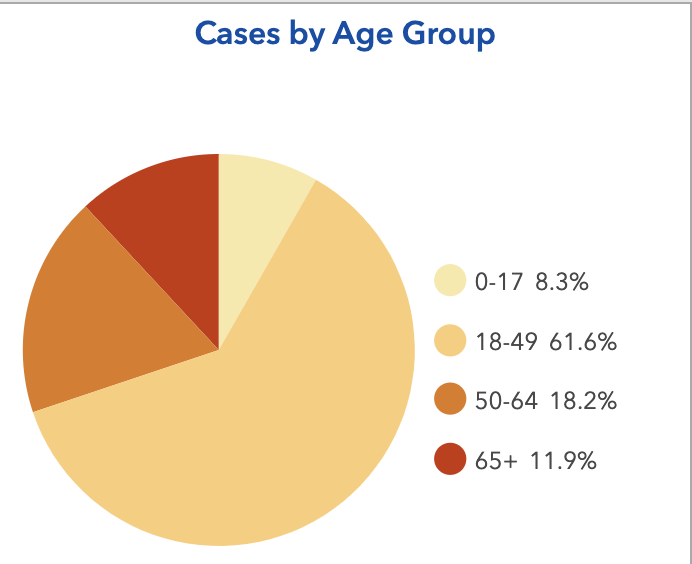
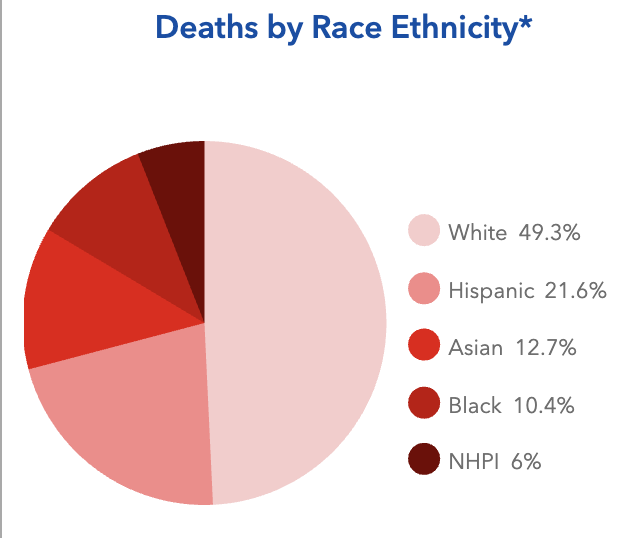
Sacramento County does a really nice job of presenting local COVID-19 data. Here is some of the current information you might find interesting.
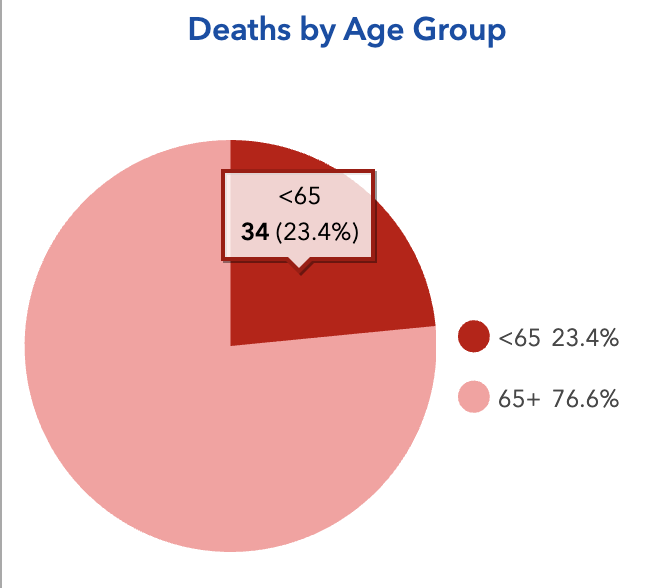
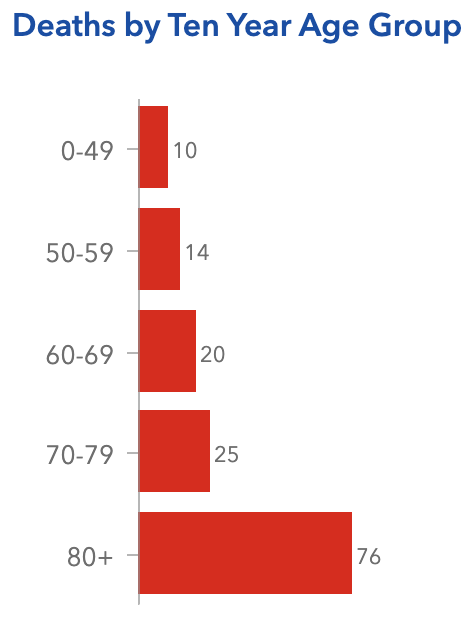
- Young people have the most cases but old people have the most deaths.
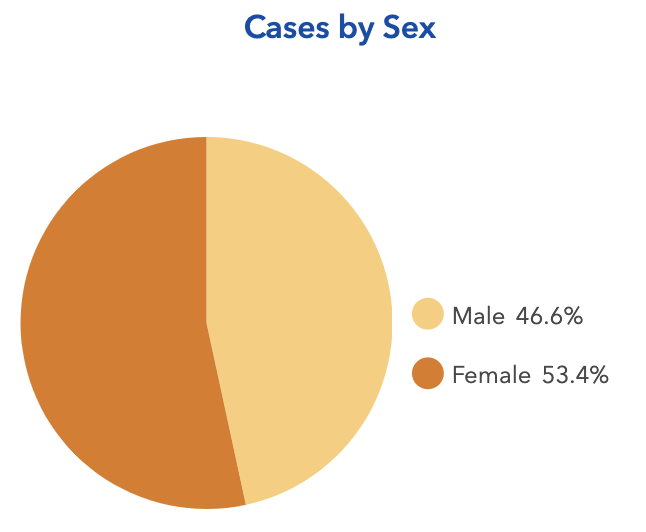
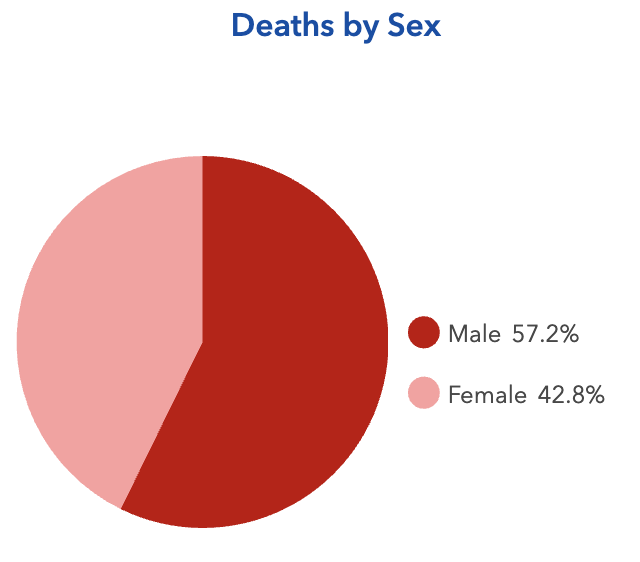
- More cases are in women but more deaths are in men.
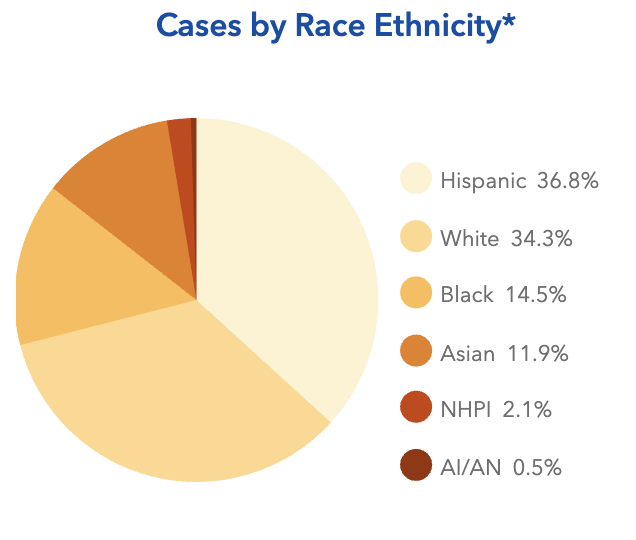
- Hispanics account for the most cases but whites account for the most deaths
Amy Rogers, MD, PhD, is a Harvard-educated scientist, novelist, journalist, and educator. Learn more about Amy’s science thriller novels, or download a free ebook on the scientific backstory of SARS-CoV-2 and emerging infections, at AmyRogers.com.
Sign up for my email list
Share this:
0 Comments